What is laryngeal cancer? Laryngeal cancer is the formation of cancerous (malignant) cells on the tissue of the larynx (voice box). The larynx is situated between our throat (pharynx) and breathing tube (trachea). Potential risk factors for the development of laryngeal cancer are: • Tobacco use • Excessive ethanol use • Male sex • Infection with human papillomavirus • Increasing age • Diets low in green leafy vegetables and/or rich in salt preserved meats and dietary fats • Metal/plastic workers • Exposure to paint, asbestos, radiation and diesel and gasoline fumes. • Laryngopharyngeal reflux Can laryngeal cancer be prevented? Adopting a healthy lifestyle could greatly reduce the risks of developing laryngeal cancer. In fact, it also reduces the chances of developing other cancers or diseases. 1) Avoid tobacco exposure Cigarettes, cigars, and other tobacco products contain carcinogens (cancer-causing substance). Hence, avoiding smoking and second-hand smoke significantly reduces risks of developing cancers. In fact, eighty-five percent (85%) of head and neck cancer is linked to tobacco use. 2) Reduce alcohol consumption Heavy alcohol intake increases the risk of laryngeal cancer. The combination of alcohol drinking and smoking increases the risk even more as alcohol increases the cancer-causing effect of tobacco smoke. 3) Healthy diet A healthy diet containing plenty of fresh fruits and vegetables, particularly tomatoes, citrus fruit and fish oil, may reduce the risk of getting laryngeal cancer. Also, avoid consuming excessive processed food and red meat. 4) Avoid chemical inhalants exposure Exposure to inhalants such as asbestos, wood dust, paint fumes, and certain chemicals, increases the risk of developing laryngeal cancer. Safety measures and precautions are needed when handling exposure to these chemicals. Laryngeal Cancer in Malaysia Incidence Summary Table, All Residence, Male, Malaysia 2007 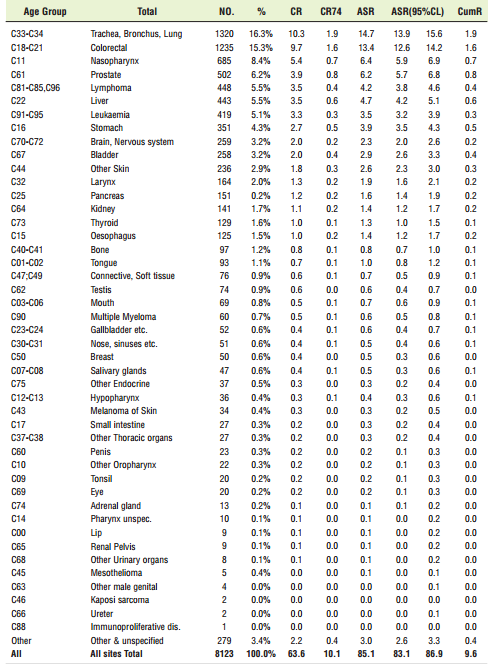 Incidence Summary Table, All Residence, Female, Malaysia 2007
Incidence Summary Table, All Residence, Female, Malaysia 2007 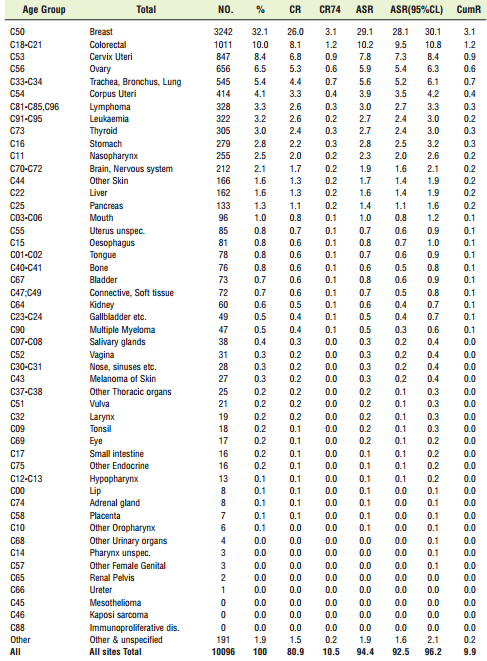 Reference: National Cancer Registry Report Malaysia Cancer Statistics – Data and Figure 2007 Symptoms of Laryngeal Carcinoma Some of the warning signs of laryngeal cancer include: 1. Hoarseness of voice / Change in your voice: Laryngeal cancers that form on the vocal cords often cause hoarseness or a change in the voice. This can lead to them being found at a very early stage. People who have voice changes (like hoarseness) that do not improve within 2 weeks should see their healthcare provider right away. 2. Lump in the neck: For cancers that don’t start on the vocal cords, hoarseness occurs only after these cancers reach a later stage or have spread to the vocal cords. These cancers are sometimes not found until they have spread to the lymph nodes and the person notices a growing mass in the neck. 3. Difficulty in swallowing: This can vary from a feeling that there is a crumb stuck in your throat to being completely unable to swallow food. You may have some pain or a burning sensation when swallowing food or you may feel that your food is stuck. A harmless narrowing of the oesophagus (called a stricture) can cause difficulty in swallowing, but it may be because a tumour or swelling is causing a blockage. Either way, you need to see your doctor and get some tests. 4. Weight loss: Weight loss is a common symptom of many cancers, including cancer of the larynx. It usually happens with more advanced cancer of the larynx and is very unlikely to be the only symptom. 5. Persistent cough: Constant irritation of the throat and feeling like you have to cough or clear your throat can be an early cancer symptom. 6. Shortness of breath: Laryngeal cancer affecting movement of vocal cords or a very extensive cancer can cause difficulty in breathing. Other less common but important symptoms include: 7. Ear pain: Sometimes pain in the throat can be felt in the ear. This is called ‘referred pain’ and can be one of the overlooked symptoms of laryngeal cancer. 8. Aspiration of fluids/food 9. Blood-tinged sputum / expectoration of tissue 10. Halitosis 11. Pain / sore throat Investigations for laryngeal carcinoma: Imaging studies:
Reference: National Cancer Registry Report Malaysia Cancer Statistics – Data and Figure 2007 Symptoms of Laryngeal Carcinoma Some of the warning signs of laryngeal cancer include: 1. Hoarseness of voice / Change in your voice: Laryngeal cancers that form on the vocal cords often cause hoarseness or a change in the voice. This can lead to them being found at a very early stage. People who have voice changes (like hoarseness) that do not improve within 2 weeks should see their healthcare provider right away. 2. Lump in the neck: For cancers that don’t start on the vocal cords, hoarseness occurs only after these cancers reach a later stage or have spread to the vocal cords. These cancers are sometimes not found until they have spread to the lymph nodes and the person notices a growing mass in the neck. 3. Difficulty in swallowing: This can vary from a feeling that there is a crumb stuck in your throat to being completely unable to swallow food. You may have some pain or a burning sensation when swallowing food or you may feel that your food is stuck. A harmless narrowing of the oesophagus (called a stricture) can cause difficulty in swallowing, but it may be because a tumour or swelling is causing a blockage. Either way, you need to see your doctor and get some tests. 4. Weight loss: Weight loss is a common symptom of many cancers, including cancer of the larynx. It usually happens with more advanced cancer of the larynx and is very unlikely to be the only symptom. 5. Persistent cough: Constant irritation of the throat and feeling like you have to cough or clear your throat can be an early cancer symptom. 6. Shortness of breath: Laryngeal cancer affecting movement of vocal cords or a very extensive cancer can cause difficulty in breathing. Other less common but important symptoms include: 7. Ear pain: Sometimes pain in the throat can be felt in the ear. This is called ‘referred pain’ and can be one of the overlooked symptoms of laryngeal cancer. 8. Aspiration of fluids/food 9. Blood-tinged sputum / expectoration of tissue 10. Halitosis 11. Pain / sore throat Investigations for laryngeal carcinoma: Imaging studies:
- CT Scan and MRI: To assess the extent of the growth, invasion into the surrounding structures and lymph nodes involvement.
- X- Ray Chest: To plan surgery and to look for distant metastasis.
- PET scan: This is a radiologic tool that detects metabolic signals from cells with high metabolic activity like cancer cells. This is the most sensitive test available to detect metastasis or second primary tumors. Currently, it is available only in a few centers in Malaysia.
Diagnostic studies:
- Direct laryngoscopy: This is the mainstay investigation needed in all patients suspected to have laryngeal carcinoma. As the patient is under general anesthesia, a detailed examination and palpation (for staging purposes and surgical planning) as well as adequate biopsies for histological confirmation are best done with this procedure.
- FNA: Fine needle aspiration of a neck mass may be done to confirm that it is a metastatic lymph node.
Treatment of Laryngeal Cancer The goals of treatment for laryngeal cancer include a complete removal of the tumor, prevention of a recurrence and preferably maintain the functions of the larynx. The treatment generally consists of:
- Radiotherapy
- Surgery (a) Conservation Laryngeal Surgery (b) Total Laryngectomy
- Combined Therapy
Early-stage tumors (Stages I-II) can be treated with either radiotherapy or laryngeal preservation surgeries. Previously, advanced tumors (Stages III-IV) were treated with total laryngectomy, reconstruction, and adjuvant postoperative chemoradiation therapy. However, remarkable progress has been made in the past 20 years in the management of laryngeal cancer. Although total laryngectomy is still required in cases of aggressive and extensive tumors, laryngeal preservation strategies using chemotherapy and radiation therapy protocols have now become the standard of care for many advanced laryngeal cancers. This emphasises the need for earlier detection and referrals to improve the prognosis.
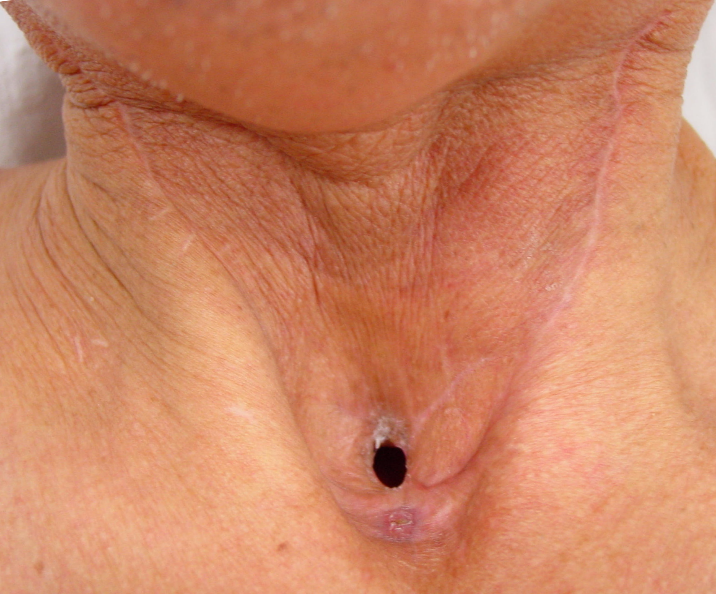
Neck of patient post-laryngectomy
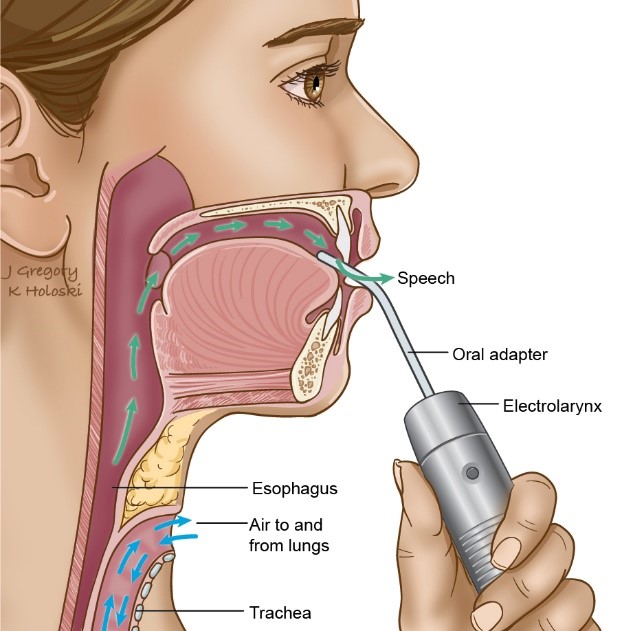
Post-laryngectomy speech rehabilitation therapy: The main limitation for patients post total laryngectomy is loss of voice. With that in view, voice restoration post-surgery is pivotal as part of the management of the patient. The method chosen depends on the communication needs of the patient, his/her physical and mental status as well the personal preference. These patients are counselled preoperatively by the surgical team along with the speech therapist for the same. There are three main options for voice restoration: 1. Electrolarynx – The most common is one that is simply held up against the skin of the neck or face and the vibrations are transmitted intra-orally. – The other type has an attachment that looks like a straw (called an oral tube) that directs the vibrations into the mouth. Vibrations of natural oral linings can result in speech, or a vibrating palatal prosthesis can result in speech. 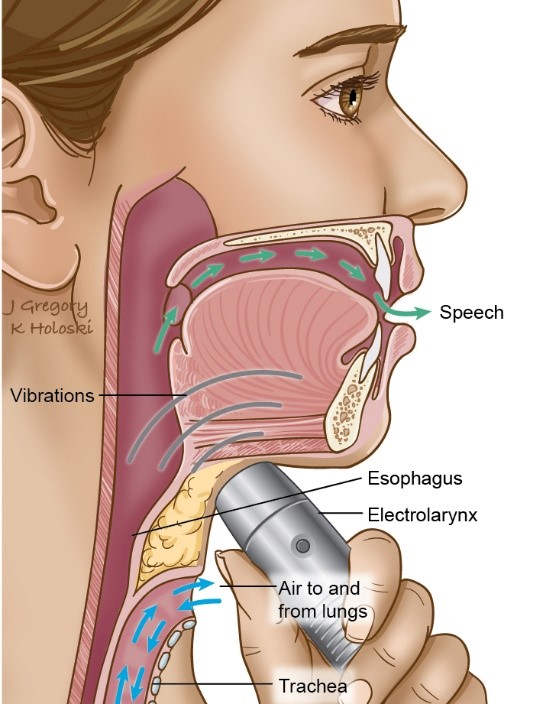
 2. Oesophageal speech – Air is trapped inside the mouth, swallowed, and then burped out. The air vibrates the surfaces of the oesophagus and pharynx to create sound.
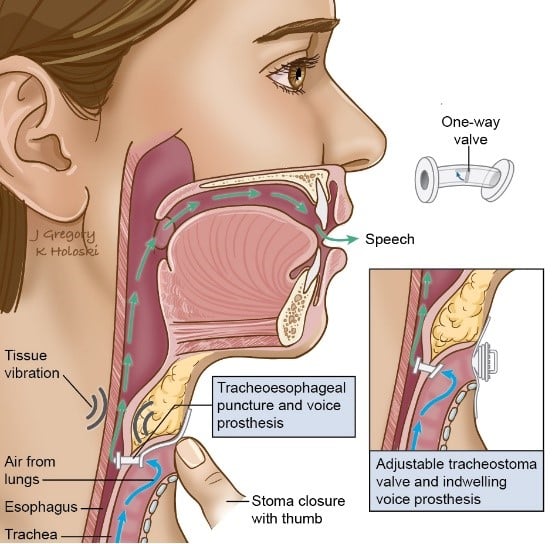
2. Oesophageal speech – Air is trapped inside the mouth, swallowed, and then burped out. The air vibrates the surfaces of the oesophagus and pharynx to create sound. 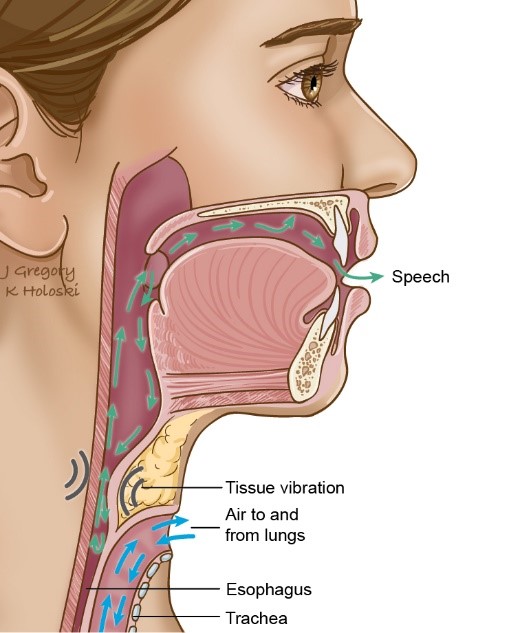 3. Trachea-oesophageal puncture with prosthesis – The TEP prosthesis has a one-way valve that allows air to go from the trachea through the prosthesis into the oesophagus – Take a breath via the trachea, then cover the tracheostomy opening in the neck when breathing out, and all the air passes through the little prosthesis that connects the trachea with the oesophagus immediately behind it. As air passes through oesophagus and pharynx, the surfaces vibrate and create sound.
3. Trachea-oesophageal puncture with prosthesis – The TEP prosthesis has a one-way valve that allows air to go from the trachea through the prosthesis into the oesophagus – Take a breath via the trachea, then cover the tracheostomy opening in the neck when breathing out, and all the air passes through the little prosthesis that connects the trachea with the oesophagus immediately behind it. As air passes through oesophagus and pharynx, the surfaces vibrate and create sound.
Prognosis of different stages of laryngeal cancer The 5-year survival rates vary depending on the treatment modality. This can range from 90% for Stage 1 glottic tumors to about 30-40% in Stage 4 tumors. Interestingly, laryngeal cancer is perhaps the only cancer to actually demonstrate a decrease in survival rates over the past few decades. The increasing use of nonsurgical therapy has been implicated in this decrease. Hence, the need is urgent for an early diagnosis and intervention. What lies in the future? The main limiting force in the treatment of these patients is the loss of voice and a permanent tracheostomy. Hence, more and more research is being conducted towards organ-preservation techniques. These mainly include better chemoradiation protocols, the use of lasers, medical targeting agents like cetuximab, immunotherapy etc. However, as of now, the best way would still be awareness, early referrals and detection for optimal treatment that can be made available for the patient. AUTHORS: 1) Leong Kai Chung, Semester 7 medical student, International Medical University 2) Ashley Ho Yann Shyan, Semester 7 medical student, International Medical University 3) Choong Shueh Cheng, Semester 7 medical student, International Medical University 4) Emily Chong Hui Xing, Semester 7 medical student, International Medical University 5) Kiran A/L Jayakumar, Semester 7 medical student, International Medical University 6) Lim Zi Qian, Semester 7 medical student, International Medical University 7) Yong Eu Ming, Semester 7 medical student, International Medical University 8) Dr Anitha Vivekanandan, Senior Lecturer (ENT), International Medical University.
Related Posts